One ecosystem, three products
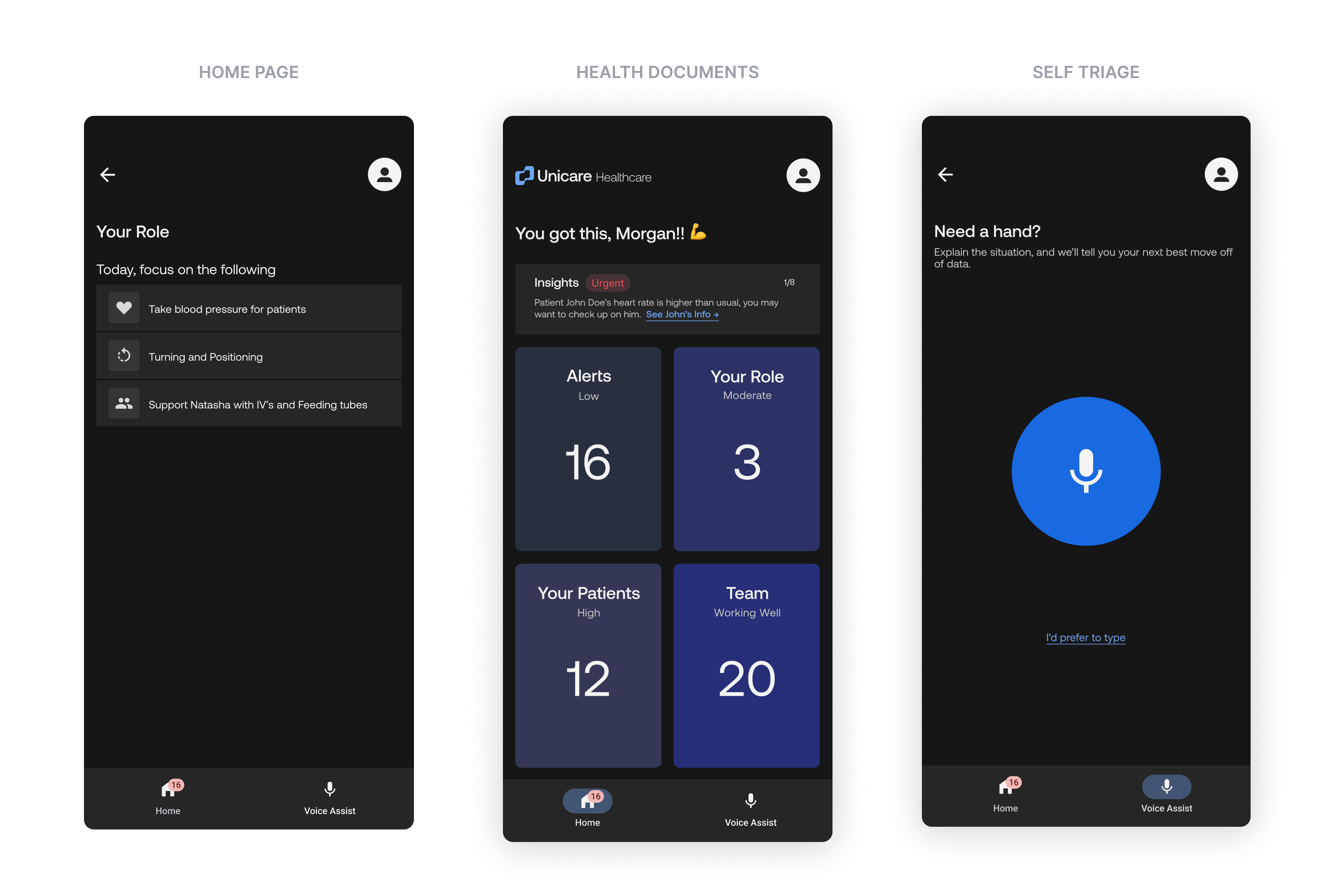
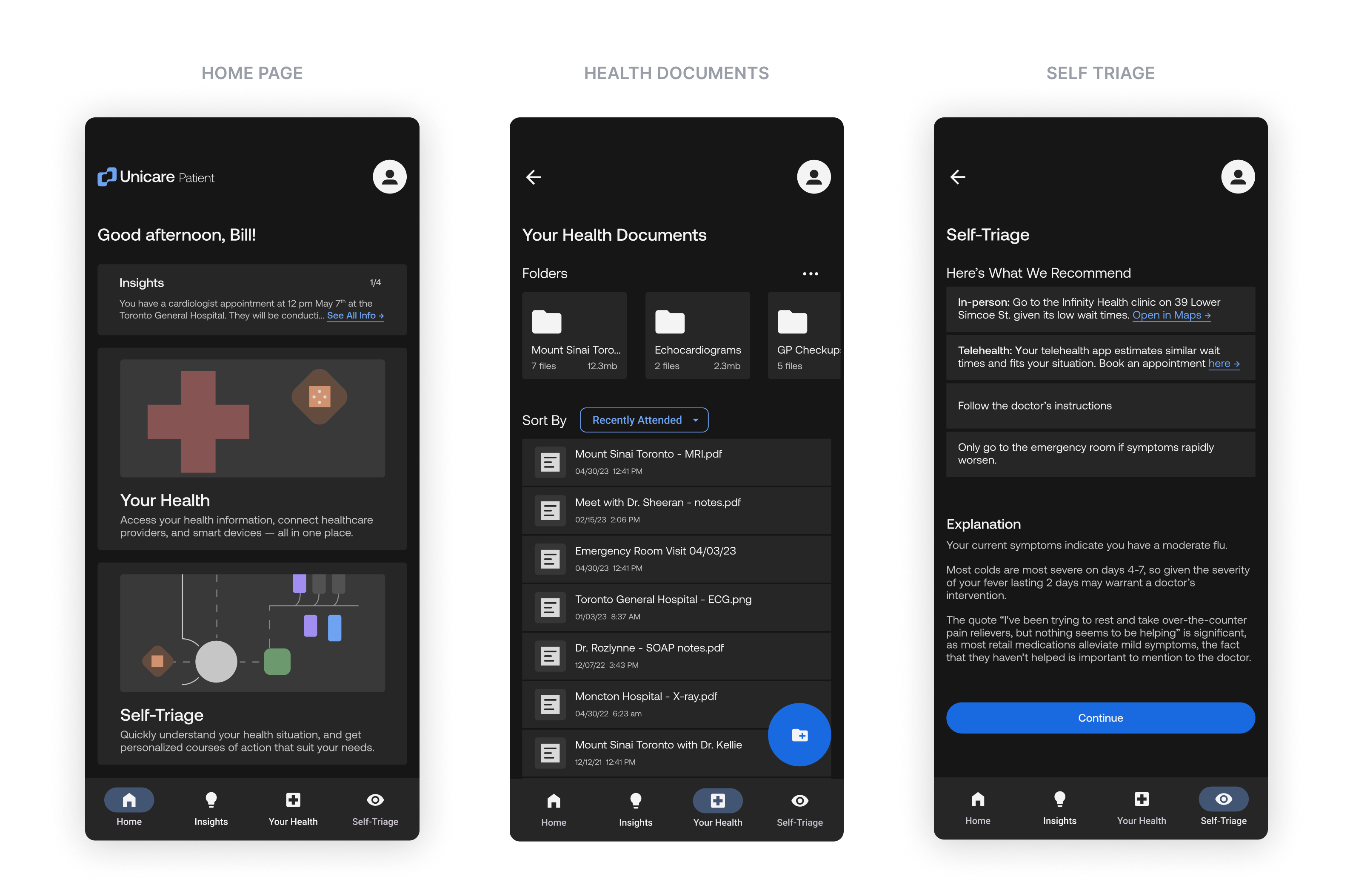
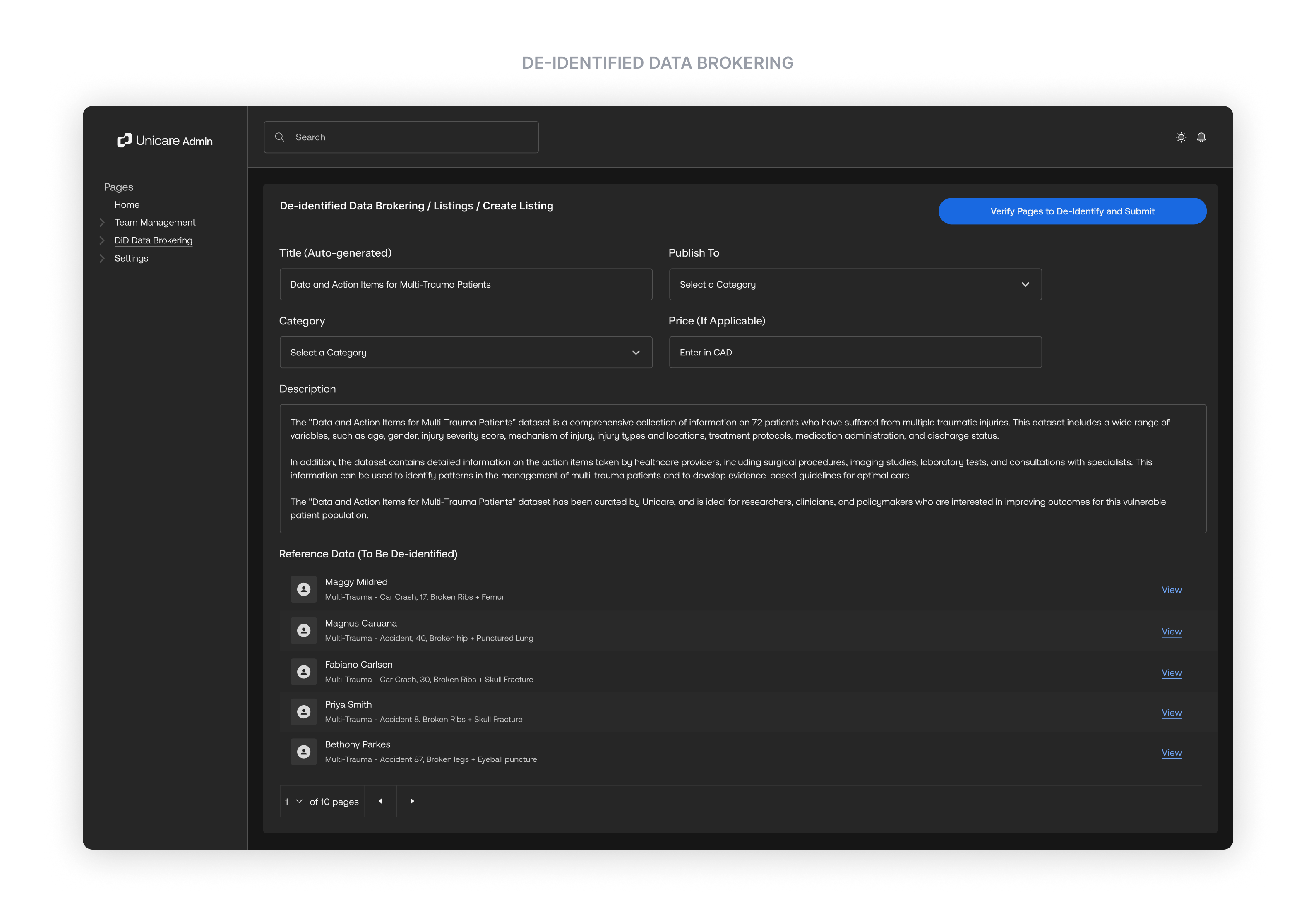
My starting thesis was that the experience for every party in Canadian healthcare was unideal, and that technology could relieve all of it if designed as one system. Instead of a single tool for a single user, I built an interconnected platform: a patient portal, a bedside decision-support app, and a management dashboard, all pulling from the same data backbone. Improvement in one creates relief across all three.

Three products connect across patients, healthcare workers, and hospital management.